ICD 10 Ocular Trauma Coding: Documentation & Shortcuts
Ocular trauma documentation must include specific clinical details to support correct diagnosis coding and timely reimbursement. ICD 10 Ocular Trauma coding depends on injury type, laterality, and encounter stage, which should be documented within 24–48 hours. Missing or incomplete documentation can delay claim processing by up to 30 days.
This blog explains documentation requirements, medical record review, coding workflow, coding shortcuts, and quick reference tables to help identify the correct ICD-10 codes for ocular trauma efficiently.
Table of Contents
Ocular Trauma ICD-10 Documentation for Faster Coding
Ocular trauma ICD-10 documentation includes clinical details required to select correct diagnosis codes. In ocular injury medical coding ICD-10, physician notes, imaging reports, and emergency documentation are completed within 24 hours, and records are reviewed within 2–3 business days.
Providers must include findings such as visual acuity (20/20, 20/40), intraocular pressure (10–21 mmHg), and imaging like CT orbit scans.
For example, ocular trauma ICD-10 codes like S05.01XA require injury type, laterality, and encounter stage. Without proper documentation, reimbursement may be delayed by 30 days.
ICD 10 Ocular Trauma Documentation Requirements
ICD 10 Ocular Trauma documentation must include specific clinical elements so that coders select the correct diagnosis code. ICD-10 coding for eye injuries requires providers to document laterality, injury cause, and encounter type. According to CMS guidelines, incomplete documentation contributes to 15–20% of coding delays.
Required documentation includes:
Injury type (abrasion, laceration, rupture)
Eye affected (right, left, bilateral)
Date of injury
Initial or follow-up encounter
Treatment performed
This supports proper ICD-10 injury coding for eye and orbit. Proper documentation of laterality also helps ensure correct code selection for other ocular conditions. Want to know the retinal detachment ICD-10 code for left, right, and bilateral eyes?
Key Elements Required in Ocular Trauma Documentation
Essential clinical elements must be clearly documented before assigning diagnosis codes. Medical coding for ocular injuries depends on injury severity, anatomical location, and encounter details. Complete documentation of these elements within the first 24–48 hours of diagnosis helps support correct code selection, reduces claim review delays, and allows proper classification of injury type and encounter stage.
Key Documentation Elements for Ocular Injury Coding
For instance, ICD-10 coding for globe rupture requires confirmation of full-thickness injury, surgical intervention, and encounter stage, as documented in operative reports or ophthalmic examination findings.
How to Review Medical Records for Ocular Injury Coding
Medical records must be reviewed in a structured order within 48–72 hours after treatment. Physician notes, diagnostic reports, and procedure summaries provide the required clinical and encounter details.
Use the following order to review records:
Review diagnosis summary
Identify injury type and affected eye structure
Confirm laterality (right, left, or bilateral)
Determine encounter stage (initial, subsequent, sequela)
Verify clinical findings and examination results
Review imaging reports such as CT or slit-lamp findings
For example, ICD-10 traumatic eye injury coding may involve multiple codes when both globe injury and orbital trauma exist. Imaging such as CT scans helps confirm ICD-10 orbital injury coding. Proper review of these records helps identify the correct injury category under the S05 classification. Check the complete list of Injury of eye & orbit S05 ICD-10 codes.
Step-by-Step Ocular Trauma Coding Using Documentation
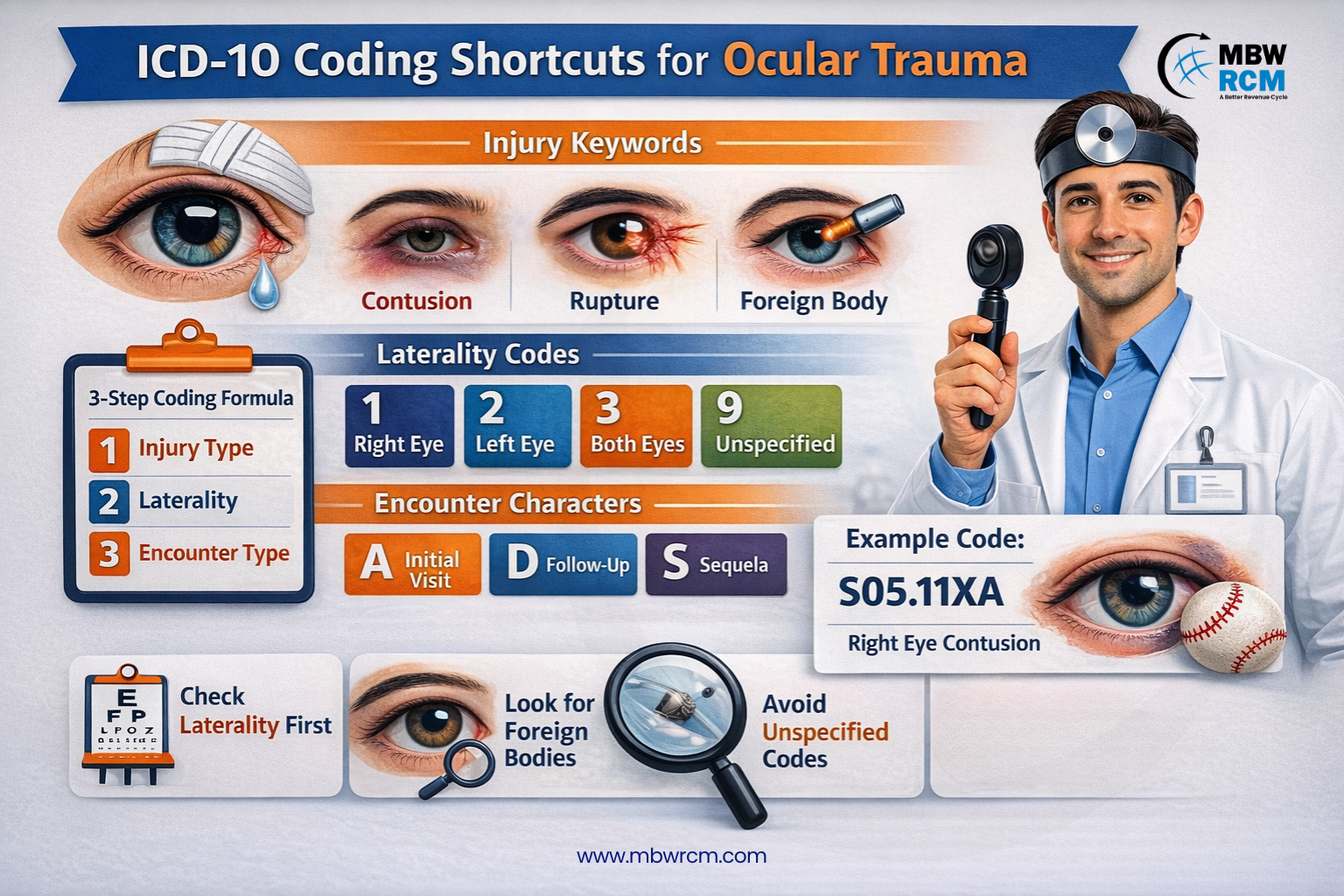
Ocular trauma coding using documentation follows a structured workflow so that injury details match the correct ICD-10-CM category and extension. ICD 10 Ocular Trauma coding begins with identifying injury type and documentation details.
Confirm the documented diagnosis and injured structure
Identify the injury type (abrasion, contusion, laceration, rupture) and the affected site (eye, cornea, orbit) from the encounter note.
Select the correct injury category
Choose the category based on documentation: injury of eye and orbit (S05), foreign body (T15), burns/corrosions (T26), or related codes.
Apply laterality from the record
Confirm right, left, bilateral, or unspecified based on exam findings and provider note. Laterality determines the correct ICD-10-CM code character and must match the documented eye affected.
Assign the encounter character
Use A for initial encounter, D for subsequent, or S for sequela, based on treatment stage documented in the record. This 7th character identifies active treatment, follow-up care, or injury-related complications.
Verify documentation support before finalizing
Cross-check supporting documentation such as slit-lamp findings, procedure summaries, or imaging reports to confirm the injury classification.
Submit the final diagnosis code set
Enter the final ICD-10-CM code(s) with the correct category, laterality, and encounter stage. Verify that the code matches the documented injury and encounter details before submission.
For example, ICD-10 contusion of eye coding requires confirmation of blunt trauma and encounter type before assigning S05.10XA.
ICD 10 Ocular Trauma Coding Shortcuts
Coding shortcuts help reduce lookup time and improve efficiency. ICD 10 Ocular Trauma shortcuts allow faster and correct code selection when documentation is complete and specific.
Apply these shortcuts to identify codes faster:
Shortcut 1: Start with the correct ICD-10 category
Use S05 for injury of eye and orbit
Use T15 for foreign body injuries
Use T26 for burns or chemical injuries
This narrows the search to the correct code group quickly
Shortcut 2: Confirm laterality before selecting the code
Identify right eye, left eye, bilateral, or unspecified
Laterality determines the correct ICD-10 code characters
Shortcut 3: Assign the correct encounter character
Use A for initial encounter
Use D for subsequent encounter
Use S for sequela
Missing the 7th character may cause claim rejection
Shortcut 4: Use the Alphabetical Index to locate codes faster
Search injury terms such as abrasion, laceration, or contusion
Then verify the code in the Tabular List
Shortcut 5: Verify documentation before final selection
Confirm injury type, affected eye, and encounter stage
This helps prevent incorrect code assignment
For instance, ICD-10 corneal foreign body code T15.01XA applies when documentation confirms foreign object in cornea. Reference tools such as Optometry Coding Cheat Sheet help locate commonly used eye injury codes faster.
Ocular Trauma Coding Quick Reference and Shortcuts Table
This quick reference table lists commonly used ocular trauma ICD-10 codes and coding shortcuts to help quickly identify the correct code based on documented injury type, laterality, and encounter stage.
Quick Lookup Table for Ocular Trauma ICD-10 Codes
For example, ICD-10 hyphema coding requires confirmation of blood accumulation and encounter stage. These shortcuts help quickly locate trauma codes, reduce lookup time, and support faster ICD-10 code selection.
Advanced Coding Shortcuts for Ocular Injury Codes
Advanced shortcuts help reduce coding time and improve consistency when handling high-volume eye injury cases. ICD 10 Ocular Trauma coding becomes faster when commonly used code patterns and documentation elements are recognized early.
Follow these advanced shortcuts:
Shortcut 1: Memorize high-frequency S05 codes
Frequently used codes include S05.01XA (right eye injury), S05.02XA (left eye injury), and S05.10XA (contusion of eyeball)
Memorizing these codes helps identify diagnosis categories faster without repeated lookup
Shortcut 2: Use EMR coding templates
Electronic Medical Record (EMR) templates highlight injury type, laterality, and encounter stage
Templates reduce manual review time and help ensure complete documentation
Shortcut 3: Maintain internal reference lists
Create quick reference sheets for common eye injuries such as abrasion, foreign body, and laceration
Internal lists help quickly match documented injuries with ICD-10 code categories
Shortcut 4: Use automated coding software tools
Coding tools suggest ICD-10 codes based on clinical documentation and diagnosis terms
These tools help reduce coding time and improve workflow efficiency
Shortcut 5: Identify injury depth and encounter stage early
Confirm whether injury is superficial, penetrating, or full-thickness
Encounter stage determines the required ICD-10 7th character
For instance, ICD-10 eye laceration coding requires identifying wound depth and encounter stage. Ophthalmology Billing Companies often implement automated workflows that reduce coding time from 5 minutes to under 90 seconds.
Conclusion
Proper documentation and correct code selection are essential for accurate ocular trauma coding and timely reimbursement. Clear clinical details such as injury type, laterality, and encounter stage help support correct ICD-10 code assignment and reduce claim delays.
Expert Ophthalmology Billing Services can help improve coding accuracy, streamline documentation review, and ensure faster claim processing. Contact MBW RCM today to learn how our billing experts can support your ocular trauma coding and documentation needs.
FAQs: Ocular Trauma ICD-10 Coding
Request for Information
Facing ICD 10 Ocular Trauma coding errors or claim denials? Expert ophthalmology coding services help improve documentation accuracy and reimbursement.
Fill out the form below to connect with a specialist and improve your ICD 10 Ocular Trauma coding efficiency.