CABG Claims Under Review: Documentation Gaps That Trigger Denials
Coronary artery bypass grafting (CABG) represents some of the most valuable procedures a cardiovascular surgery practice performs—and some of the most closely reviewed by payers. Between multiple grafts, complex coding rules, assistant surgeon reporting, and detailed operative documentation, even a small documentation gap can create payment delays that no practice wants to deal with.
In many cases, a denied CABG claim isn't the result of incorrect coding alone. The surgery may have been performed flawlessly, but if the documentation doesn't clearly support what was done, payers may request additional records, delay reimbursement, or deny the claim altogether.
Table of Contents
As reimbursement scrutiny continues to increase, accurate documentation has become just as important as accurate coding. Understanding where documentation gaps commonly occur can help cardiovascular practices improve clean claim rates, reduce avoidable denials, and protect revenue from every CABG procedure.
Why CABG Claims Receive Greater Payer Scrutiny
CABG procedures are inherently complex. They often involve multiple grafts, harvested vessels, assistant surgeons, and extensive operative reports—all of which must align with the services billed.
Because these procedures carry significant reimbursement value, payers typically review them more carefully than many routine surgical claims. Incomplete documentation can raise questions about medical necessity, coding accuracy, or whether the billed services are fully supported by the clinical record.
CMS continues to evaluate CABG through episode-based cost measures that span a 30-day period before surgery and a 90-day period after surgery, highlighting the importance of complete documentation throughout the patient's episode of care. Practices participating in Medicare quality programs should pay close attention to documentation consistency across the entire revenue cycle.
Learn more about CABG episode-based measures through the CMS Quality Payment Program here.
"The operative report should clearly document the procedure performed and support the services billed."
— Centers for Medicare & Medicaid Services (CMS)
Documentation Gap #1: The Number of Grafts Isn't Clearly Documented
It may seem like a small detail, but documenting the exact number of grafts is one of the first things payers look for.
If the operative report doesn't clearly support the number of grafts billed, the claim can quickly end up under review or require additional documentation before payment is released.
The operative report should clearly identify:
Total number of grafts performed
Each target coronary artery
Conduit used for each graft
Sequential grafts, when applicable
Any revisions or additional bypasses performed
Even a simple inconsistency between the operative report and the coded claim can delay reimbursement.
Documentation Gap #2: Arterial vs. Venous Graft Details Are Missing
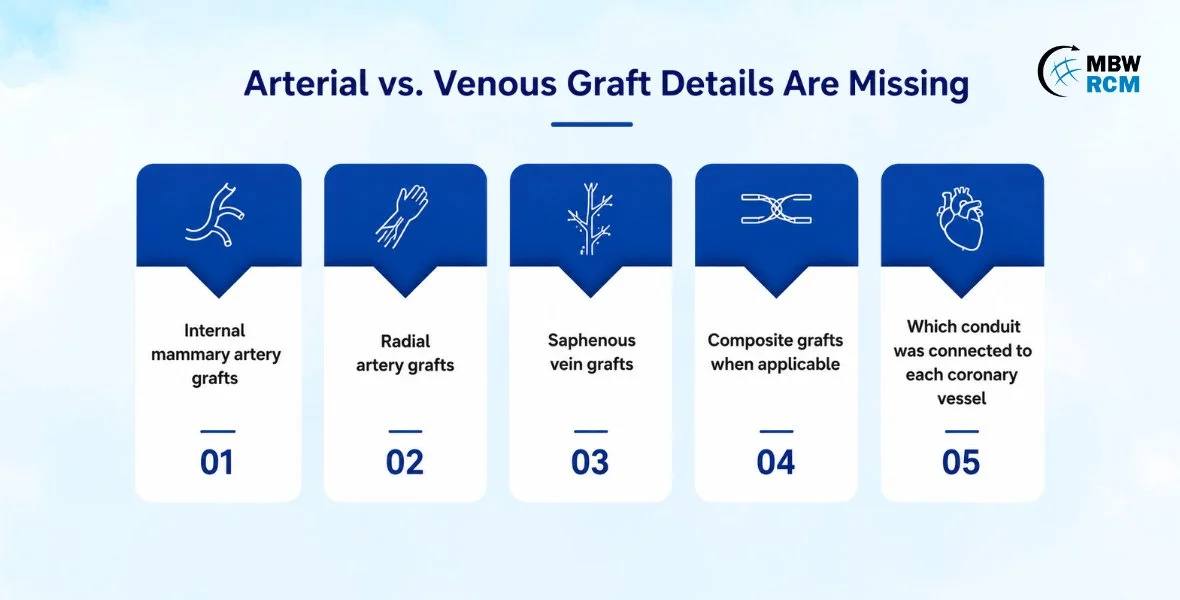
Not all grafts are reported the same way, which makes this section of the operative report especially important.
Whether the surgeon used an internal mammary artery, radial artery, or saphenous vein should be clearly documented so coding accurately reflects the procedure performed.
Documentation should identify:
Internal mammary artery grafts
Radial artery grafts
Saphenous vein grafts
Composite grafts when applicable
Which conduit was connected to each coronary vessel
When these details are missing, coders may have difficulty selecting the appropriate CPT® codes, increasing the likelihood of payer edits or documentation requests. To learn more about coding accuracy and reimbursement for cardiovascular procedures, read Medical Billing for Cardiovascular Coding Simplified.
Documentation Gap #3: Harvest Documentation Often Falls Short
Harvest documentation is another area that's frequently overlooked.
When details about how the vessel was harvested—or even which vessel was harvested—are missing, coders are left filling in the blanks, and that's never a good position to be in.
A complete operative report should document:
Vessel harvested
Harvest technique
Open or endoscopic approach
Laterality when applicable
Separate incision details
Clinical necessity for the harvest
Clear documentation not only supports coding accuracy but also helps defend the claim if it's selected for medical review.
Documentation Gap #4: Add-On Code Sequencing Errors
CABG coding rarely involves just one procedure code.
Multiple grafts often require add-on codes, and those codes must be reported in the proper sequence. A simple sequencing error can trigger payer edits even when every procedure was appropriately documented and performed.
Common mistakes include:
Incorrect primary procedure selection
Missing add-on codes
Reporting add-on codes independently
Improper sequencing
Documentation that doesn't fully support additional grafts
Reviewing code sequencing before claim submission can prevent unnecessary payment delays.
Documentation Gap #5: Operative Reports Lack the Detail Payers Expect
Think of the operative report as the roadmap for the entire claim.
If key clinical details are missing or unclear, payers have little reason to assume what was done. That's when additional documentation requests—or worse, denials—begin to appear.
A strong CABG operative report should include:
Surgical indication
Coronary vessels bypassed
Number of proximal and distal anastomoses
Conduit selection
Cardiopulmonary bypass usage
Surgical techniques performed
Intraoperative findings
Completion status of the procedure
The more complete the operative report, the easier it becomes to support both coding accuracy and reimbursement.
Documentation Gap #6: Global Surgical Period Issues
Reimbursement challenges don't always stop once the surgery is over.
Follow-up visits, return-to-the-operating-room procedures, and unrelated services billed during the global period all have specific documentation requirements. Missing those details can create avoidable reimbursement issues long after the initial CABG claim has been processed.
Practices should carefully review:
Postoperative E/M documentation
Modifier usage
Return-to-OR procedures
Unrelated postoperative services
Global surgical package rules
Getting these details right helps prevent denials that occur well after the surgery itself. If you're interested in learning more about cardiovascular billing, take a look at this article on TAVR Billing & Coding: Protect High-Value Claims.
Documentation Gap #7: Assistant Surgeon Reporting
Reporting an assistant surgeon isn't as simple as adding the appropriate modifier.
Payers generally want to understand why an assistant was medically necessary and what role they played during the procedure. If that information isn't reflected in the operative report, reimbursement may be reduced—or denied entirely.
Documentation should support:
Medical necessity
Specific responsibilities performed
Assistant participation within the operative report
Appropriate modifier selection
Payer-specific assistant surgeon requirements
Documentation Gap #8: Medical Necessity Isn't Fully Supported
Even technically accurate claims can be questioned if the clinical documentation doesn't clearly establish why CABG was necessary.
Supporting documentation should include:
Coronary angiography findings
Severity of coronary artery disease
Patient symptoms
Previous treatment history
Failed conservative therapy when appropriate
Clinical decision-making supporting surgery
Medical necessity documentation often determines whether a high-value CABG claim moves smoothly through adjudication or ends up in medical review.
Best Practices to Reduce CABG Claim Denials
Strong documentation starts well before the claim reaches the payer.
Practices that consistently perform well with CABG reimbursement often have standardized documentation and coding workflows that reduce variation between surgeons, coders, and billers.
Some best practices include:
Standardize CABG operative report templates.
Verify graft counts before coding.
Clearly document conduit types.
Capture complete harvest details.
Review add-on code sequencing before submission.
Validate assistant surgeon documentation.
Confirm modifier usage.
Perform regular coding audits.
Monitor payer-specific denial trends.
Educate providers as documentation requirements evolve.
These small process improvements can make a measurable difference in reimbursement performance over time.
CABG Documentation Checklist Before Claim Submission
Before submitting a CABG claim, verify that the record includes:
✔ Total number of grafts
✔ Arterial versus venous conduit identification
✔ Harvest technique documented
✔ Target coronary arteries identified
✔ Complete operative report
✔ Correct CPT® sequencing
✔ Assistant surgeon documentation
✔ Appropriate modifiers
✔ Medical necessity supported
✔ Global surgical period reviewed
Industry Perspective
According to CMS, Medicare tracks submitted services, allowed services, denied services, and payment information for physician procedures every year. High-value cardiovascular procedures remain an important area for documentation accuracy because incomplete records can affect reimbursement, compliance, and audit outcomes.
Additional Medicare procedure summary information is available → Click here to read more.
"Documentation should be clinically meaningful while supporting accurate coding and reimbursement."
— American Medical Association (AMA)
The AMA has consistently emphasized that quality documentation should accurately reflect the patient's clinical story while providing the information necessary for compliant coding and billing.
Learn more about the AMA's documentation guidance.
Conclusion
Every CABG procedure requires precision in the operating room, and the billing process deserves the same level of attention.
When documentation clearly supports the services performed, coding becomes more accurate, claims move through payers more efficiently, and practices spend less time addressing preventable denials. Even small documentation gaps—such as graft details, harvest techniques, or operative report specificity—can significantly affect reimbursement.
Partnering with experienced Cardiovascular Surgery Billing Services helps practices strengthen documentation, improve coding accuracy, reduce denials, and protect revenue on every CABG claim.
FAQs: CABG Claims Under Review & Documentation Gaps
Protect Every CABG Claim Before It Reaches the Payer
Every denied CABG claim represents revenue your practice has already earned—but may not receive without additional work.
Our cardiovascular surgery billing specialists review operative documentation, coding accuracy, and payer-specific requirements to help practices reduce denials, strengthen compliance, and maximize reimbursement for every CABG procedure.