TAVR Billing and Coding: Why High-Value Claims Lose Reimbursement
Every Transcatheter Aortic Valve Replacement (TAVR) procedure represents a significant investment in clinical expertise, advanced technology, and patient care. It also represents one of the highest-value claims a cardiovascular practice will submit. Yet, many practices don't lose revenue because the procedure wasn't performed correctly—they lose it because the billing process falls short.
TAVR billing is far more complex than submitting a standard cardiovascular claim. Multiple providers may be involved, expensive implantable devices must be captured accurately, payer policies vary, and documentation requirements leave little room for error. A missed modifier, incomplete operative report, or overlooked payer edit can delay reimbursement for weeks or even months.
Table of Contents
According to the STS/ACC TVT Registry, TAVR volumes have increased significantly over the past decade as indications expanded to lower-risk patients, making reimbursement accuracy increasingly important for structural heart programs. Likewise, the Centers for Medicare & Medicaid Services (CMS) maintains specific National Coverage Determination (NCD) requirements that directly influence reimbursement for eligible TAVR procedures.
If your practice performs TAVR procedures, understanding where high-value claims commonly lose reimbursement can help you reduce denials, improve cash flow, and protect revenue.
Why TAVR Billing Is More Complex Than Traditional Cardiovascular Procedures
Unlike many cardiovascular procedures, TAVR involves multiple moving parts that must align for successful reimbursement.
A single case may include interventional cardiologists, cardiothoracic surgeons, anesthesiologists, imaging specialists, hospitals, and device manufacturers. Each contributes to the episode of care, but each also creates additional billing complexity.
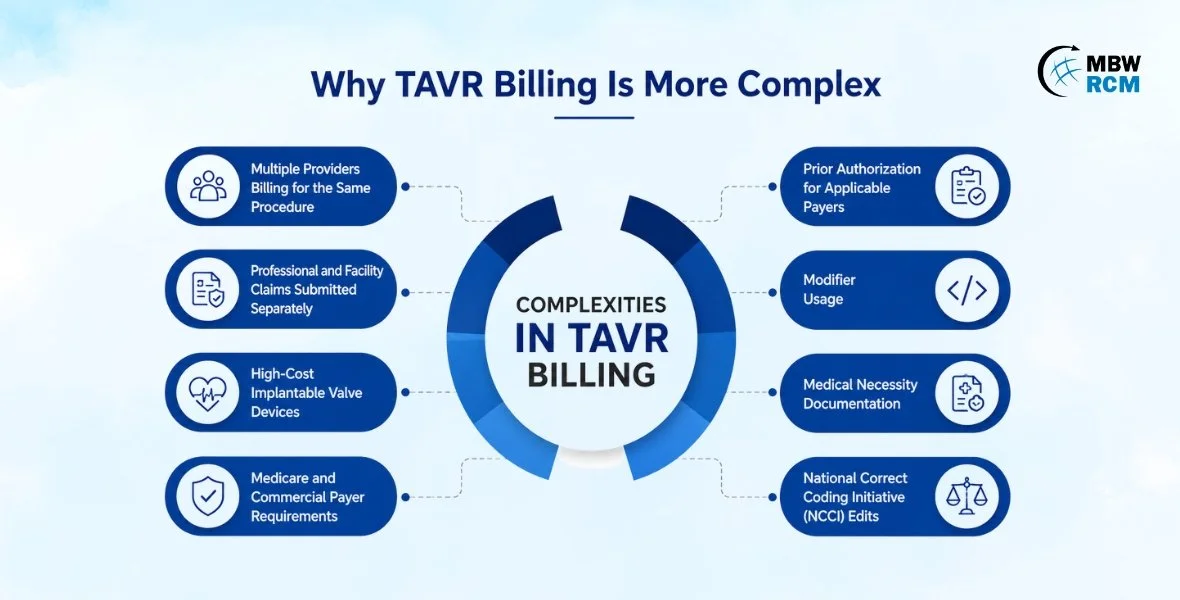
Some of the biggest challenges include:
Multiple providers billing for the same procedure
Professional and facility claims submitted separately
High-cost implantable valve devices
Medicare and commercial payer requirements
Prior authorization for applicable payers
Modifier usage
Medical necessity documentation
National Correct Coding Initiative (NCCI) edits
Because reimbursement amounts are substantial, payers typically review these claims more carefully than lower-value procedures.
"The highest-value cardiovascular claims often require the highest level of billing precision."
Professional Billing vs. Facility Billing: Know the Difference
One of the biggest sources of confusion in TAVR reimbursement is understanding the distinction between professional and facility billing.
Although both relate to the same procedure, they are processed separately and have different documentation and reimbursement requirements.
Professional Billing
Professional billing covers physician services, including:
Surgeon or interventional cardiologist services
Evaluation and Management (E/M) visits
Procedural work
Interpretation of diagnostic studies
Follow-up care
Professional claims rely heavily on physician documentation, CPT coding, modifiers, and medical necessity.
Facility Billing
Facility billing reflects the hospital's resources used during the procedure, including:
Operating or hybrid procedure room
Nursing care
Imaging equipment
Cath lab resources
Recovery services
Implantable valve device
Medical supplies
While these claims are billed separately, payers often review them together for consistency. Discrepancies between physician and facility documentation can trigger additional review or payment delays.
Assistant Surgeon Reporting: A Common Source of Denials
Assistant surgeon services are frequently reviewed by payers because they must be medically necessary and properly documented.
Many denials occur because practices assume an assistant surgeon can automatically bill for participation. In reality, reimbursement depends on payer policy, clinical necessity, and documentation supporting why assistance was required.
Documentation should clearly explain:
The assistant surgeon's role
Why assistance was medically necessary
Services performed during the procedure
Compliance with payer billing requirements
Missing or incomplete documentation often results in denied or reduced reimbursement.
Co-Surgeon Documentation Requires Clear Responsibility
Some TAVR procedures involve both a cardiothoracic surgeon and an interventional cardiologist working together.
While co-surgeon billing may be appropriate, documentation must clearly distinguish each physician's contribution.
Best practices include:
Separate Operative Documentation
Each physician should document the services personally performed rather than relying on duplicated operative notes.
Clearly Defined Responsibilities
Documentation should identify which portion of the procedure each physician completed.
Consistent Clinical Records
Physician documentation should align with the facility record to avoid inconsistencies that may prompt payer review.
When documentation overlaps or lacks specificity, reimbursement can be delayed while payers determine whether services were billed appropriately.
Device-Related Charges Can Significantly Affect Reimbursement
One of the most valuable components of a TAVR procedure is the implanted valve itself.
If device-related charges are incomplete, inaccurate, or improperly documented, hospitals risk substantial revenue leakage.
Common issues include:
Missing implant documentation
Incorrect charge capture
Device inventory discrepancies
Billing errors related to implant tracking
Inconsistent documentation between clinical and billing records
Because implant costs represent a significant portion of facility reimbursement, strong charge capture processes are essential.
Prior Authorization Still Matters
While Medicare follows its own coverage requirements, many commercial insurers require prior authorization before a TAVR procedure is performed.
Authorization issues commonly include:
Missing approvals
Expired authorizations
Incorrect procedure details
Missing clinical documentation
Changes to the treatment plan after approval
These issues don't always lead to outright denials, but they frequently delay reimbursement while additional information is requested.
Verifying authorization early in the scheduling process helps prevent avoidable payment delays.
Site-of-Service Rules Can Influence Payment
Not every payer reimburses TAVR procedures the same way.
The site where care is delivered can directly affect coverage and payment.
Hospital Inpatient
Most TAVR procedures continue to be performed in qualified hospitals with structural heart programs.
Hospital Outpatient
Some payer policies include specific outpatient reimbursement considerations depending on patient status and clinical circumstances.
Observation Status
Patient classification can influence reimbursement and documentation requirements, making accurate status assignment important.
Understanding payer-specific site-of-service rules helps practices avoid billing discrepancies and unexpected reimbursement issues.
Common Payer Edits That Delay TAVR Claims
Even when documentation is complete and coding is accurate, automated payer edits can still delay reimbursement.
Some of the most common edits include:
Medical Necessity Edits
Claims lacking sufficient clinical documentation may be flagged for review.
NCCI Edits
National Correct Coding Initiative edits evaluate whether billed services should be reported separately.
Modifier Edits
Incorrect or missing modifiers remain a leading cause of delayed physician reimbursement.
Duplicate Claim Edits
Professional and facility claims submitted inconsistently may trigger duplicate claim reviews.
Documentation Edits
Missing operative reports, physician signatures, or supporting records often lead to requests for additional documentation.
Regular denial analysis helps practices identify recurring payer edit trends before they become larger revenue cycle problems.
Best Practices to Protect Every High-Value TAVR Claim
Successful cardiovascular practices take a proactive approach to reimbursement rather than waiting for denials to occur.
Consider implementing these best practices:
Verify insurance eligibility before every procedure.
Confirm payer-specific authorization requirements.
Strengthen physician documentation.
Review coding and modifier accuracy.
Validate device-related charges.
Perform routine coding audits.
Monitor payer edits and denial trends.
Reconcile payments to identify underpayments.
Educate providers and billing staff on evolving payer policies.
Small improvements throughout the billing process can have a measurable impact on overall reimbursement. Strengthen physician documentation and follow the recommendations in our Medical Billing for Cardiovascular Coding Simplified guide to improve claim quality and reimbursement accuracy.
How Specialty Cardiovascular Billing Teams Reduce Revenue Leakage
TAVR billing requires more than general medical billing knowledge. It demands an understanding of structural heart procedures, evolving reimbursement policies, documentation expectations, and payer behavior.
Specialty cardiovascular billing teams help practices by:
Improving coding accuracy
Reviewing documentation before claim submission
Managing prior authorization workflows
Identifying underpayments
Appealing denied claims
Monitoring payer trends
Optimizing revenue cycle performance
Instead of reacting to reimbursement problems after they occur, practices can address potential issues before claims ever reach the payer. Want to learn more about cardiovascular billing? Check out this guide on Cardiovascular Stress Testing Billing & Coding.
"Every denied claim tells a story. More often than not, that story begins long before the claim reaches the payer."
Conclusion
TAVR procedures are among the most valuable—and most closely scrutinized—claims submitted by cardiovascular practices. While clinical teams focus on delivering exceptional patient outcomes, billing teams face the equally important responsibility of ensuring every claim accurately reflects the care provided.
From distinguishing professional and facility billing to documenting co-surgeons, capturing device-related charges, meeting prior authorization requirements, and navigating payer edits, every step in the revenue cycle influences reimbursement.
The encouraging news is that most reimbursement issues are preventable. Strong documentation, specialty coding expertise, proactive claim reviews, and continuous revenue cycle monitoring can dramatically reduce denials while protecting the revenue your practice has earned.
Practices that treat billing with the same level of precision they apply to patient care are far better positioned to improve cash flow, reduce administrative burden, and maximize reimbursement for every TAVR procedure.
FAQs: TAVR Billing and Coding
Request a TAVR Claim Review
Every delayed, denied, or underpaid TAVR claim represents revenue your practice has already earned.
Our cardiovascular billing specialists review your documentation, coding accuracy, payer edits, device charge capture, and reimbursement trends to identify hidden revenue opportunities and reduce preventable payment delays.
Request a TAVR Claim Review and discover how your practice can improve reimbursement, strengthen compliance, and protect every high-value cardiovascular claim.