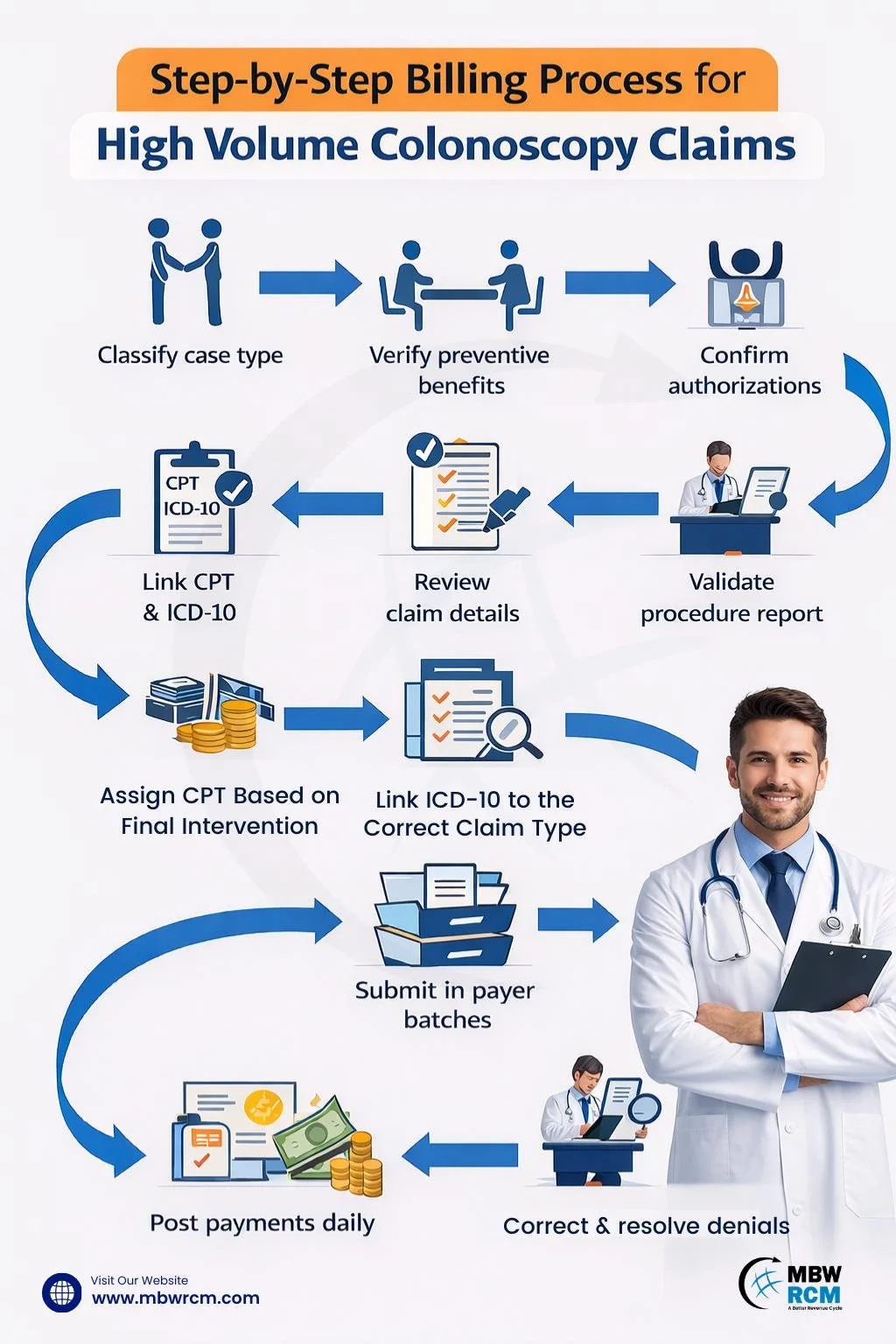
Gastroenterology Medical Billing Process for Handling High Volume Colonoscopy Claim
Gastroenterology medical billing for handling high volume colonoscopy claims requires structured coordination from scheduling to denial resolution. When a GI center performs 25–60 colonoscopies per day, even a 3% coding error rate can create dozens of rework cases weekly. Therefore, a standardized framework helps stabilize high volume colonoscopy billing, reduce denials, and support predictable reimbursement cycles across payers.

This guide explains how gastroenterology practices can manage high volumes of colonoscopy claims efficiently, detailing the workflow and controls required to maintain stable billing performance and consistent reimbursement.
Table of Contents
Step 1: Classify Colonoscopy Cases Before the Procedure
The first control point in Gastroenterology medical billing is correct classification. Every scheduled case should be labeled as screening, diagnostic, or therapeutic at least 48 hours prior to the procedure date.
This early classification prevents preventive-to-diagnostic confusion and aligns the Colonoscopy billing process with payer policy before documentation reaches coding.
Step 2: Verify Preventive Benefits and Frequency Limits
Preventive screening colonoscopy is often covered once every 10 years under Medicare guidelines. However, commercial plans may apply different intervals.
During high volume colonoscopy billing cycles, eligibility verification should confirm:
Deductible status
Coinsurance rules
Frequency limitations
Preventive coverage indicators
This verification step protects the Colonoscopy reimbursement process from avoidable patient balance disputes.
Step 3: Confirm Authorization for Diagnostic and Therapeutic Cases
Diagnostic colonoscopy and therapeutic procedures such as polypectomy or EMR frequently require authorization. Missing authorization can delay payment by 30–60 days.
For example, when billing a colonoscopy with emr cpt code, payers often require prior approval documentation. Authorization numbers must match rendering provider, facility NPI, and date of service to maintain claim validity.
Step 4: Identify Screening-to-Diagnostic Conversion Status
Screening-to-diagnostic conversion remains one of the most common causes of denial in High volume colonoscopy billing. To better understand this classification difference, refer to this guide on GI billing screening vs diagnostic.
If biopsy or polyp removal occurs, documentation must clearly support the shift. The Colonoscopy claim submission process must reflect the appropriate modifier pathway based on payer rules to prevent preventive claim misprocessing.
Step 5: Validate the Colonoscopy Procedure Report Before Coding
proper documentation drives Gastroenterology coding and billing efficiency. The colonoscopy report must include:
Indication
Extent reached (cecum confirmation)
Findings
Intervention performed
Specimen collection
Incomplete documentation delays coding by 24–48 hours and increases denial risk within the Endoscopy billing process.
Step 6: Assign CPT Based on Final Intervention
Coding should reflect the highest level of intervention performed, not the original intent. In high volume colonoscopy billing, small CPT errors can increase denial rates by 5–10%.
Coders should review the operative report to confirm biopsy, snare removal, ablation, bleeding control, or EMR. Each added intervention affects reimbursement and may trigger NCCI edits.
Proper CPT selection also affects RVU calculation, facility reimbursement, and modifier application within the colonoscopy claim workflow.
Common Colonoscopy CPT Codes Used in High Volume Billing
The cpt code for endoscopy and colonoscopy must match documentation to prevent bundling edits. Gastroenterology CPT Codes should be reviewed weekly in high volume settings to reduce repetitive coding errors.
Step 7: Link ICD-10 to the Correct Claim Type
Diagnosis selection determines medical necessity validation. In high volume colonoscopy billing, ICD-10 codes must match the documented indication and findings.
A mismatch between procedure intent and diagnosis can trigger medical necessity denials within 7–14 days of adjudication. Screening, diagnostic, and findings-based cases should follow separate coding pathways to maintain clean claim performance.
Claim Type–Specific ICD-10 Code Reference
Proper linkage strengthens the Colonoscopy reimbursement process and reduces medical necessity denials.
Step 8: Apply Required Colonoscopy Modifiers
Modifier errors account for nearly 20% of GI billing denials in high procedure environments. Preventive indicators and professional/technical split billing must follow payer rules. Practices should reference the official CMS Colonoscopy Billing & Coverage Guidelines to align modifier usage with current coverage policies.
Correct modifier application supports Colonoscopy billing for GI practices managing daily case volumes above 40 procedures.
Step 9: Perform a Colonoscopy-Specific Claim Review Before Submission
In high volume colonoscopy billing, final review prevents avoidable clearinghouse rejections. Small data errors can delay processing by 24–48 hours. A focused colonoscopy claim management check helps control repeat mistakes across large daily batches.
Before submission, review:
CPT and ICD linkage
Authorization number
Place of service
Rendering NPI
Modifier accuracy
A structured review reduces clearinghouse rejection rates by up to 15% in structured Colonoscopy claim management systems.
Step 10: Submit Claims in Organized Payer Batches
Batch submission grouped by payer improves tracking and reconciliation. High-performing GI centers submit claims within 24 hours of service.
An organized Colonoscopy claim submission process reduces average days-to-acknowledgment to less than 48 hours.
Step 11: Correct Rejections Within 24 Hours
Clearinghouse rejections should be corrected the same day or within one business day. Delayed corrections can affect timely filing limits, which range from 90 to 180 days depending on payer.
Rapid correction maintains efficiency in GI revenue cycle management workflows.
Step 12: Post Payments and Compare Expected Rates
Payment posting should occur daily. Compare contracted reimbursement rates against ERA payments to identify underpayments.
Regular reconciliation strengthens the Colonoscopy reimbursement process and protects revenue across high volume claim cycles.
Step 13: Resolve Denials by Category
In high volume colonoscopy billing, denial handling should be organized to avoid repeated rework and delays. Grouping denials by type helps identify patterns and correct issues faster. Denied colonoscopy claims should be grouped into categories:
Preventive mismatch
Missing authorization
Modifier errors
Medical necessity
Bundling edits
Structured denial categorization improves resolution turnaround from 30 days to under 14 days in optimized systems.
Step 14: Monitor Weekly Colonoscopy Billing Metrics
Tracking performance is essential in Gastroenterology medical billing environments handling high procedure volumes.
Key Gastroenterology KPIs include:
Clean claim rate (target: 95%+)
Denial rate (target: <5%)
Days in A/R (target: <35 days)
First-pass resolution rate (target: 90%+)
Technology supported by Gastroenterology EMR integration improves reporting accuracy. Some practices partner with a Gastroenterology Billing Company to manage volume spikes and maintain compliance.
How to Improve Clean Claim Rates for High Volume Colonoscopy Claims
Improving clean claim rates requires standardization across the entire Gastroenterology medical billing workflow.
Best-performing GI practices:
Audit 10% of colonoscopy cases weekly
Re-train coders quarterly on CPT Codes for Gastroenterology
Automate eligibility checks 72 hours prior to procedures
Monitor denial patterns monthly
Review modifier use for screening-to-diagnostic cases
Compare top CPT reimbursements with payer contracts quarterly
When documentation clarity, coding precision, and authorization tracking align, clean claim rates consistently exceed 95%, even in centers performing 1,000+ colonoscopies per month.
Upgrade Your Gastroenterology Medical Billing Performance
High volume colonoscopy claim handling within Gastroenterology billing depends on classification precision, preventive verification, authorization tracking, CPT and ICD alignment, modifier consistency, structured submission, and systematic denial monitoring. By implementing a step-driven workflow supported by GI revenue cycle management systems, gastroenterology practices can stabilize reimbursement and maintain operational efficiency during peak colonoscopy volumes.
High volume colonoscopy claims demand structured Gastroenterology medical billing workflows to protect reimbursement. Optimize your GI revenue cycle today—Contact MBW RCM for expert support.
FAQs: High Volume Colonoscopy Claim in Gastroenterology Billing
Request for Information
Billing errors and delays can impact reimbursement for high-volume colonoscopy claims.
Strengthen your Gastroenterology Medical Billing Process for Handling High Volume Colonoscopy Claim to reduce denials and improve cash flow. Fill out the form below to connect with a specialist and improve your GI billing performance.