5 Outpatient Billing Rules That Govern Family Practice Billing Codes

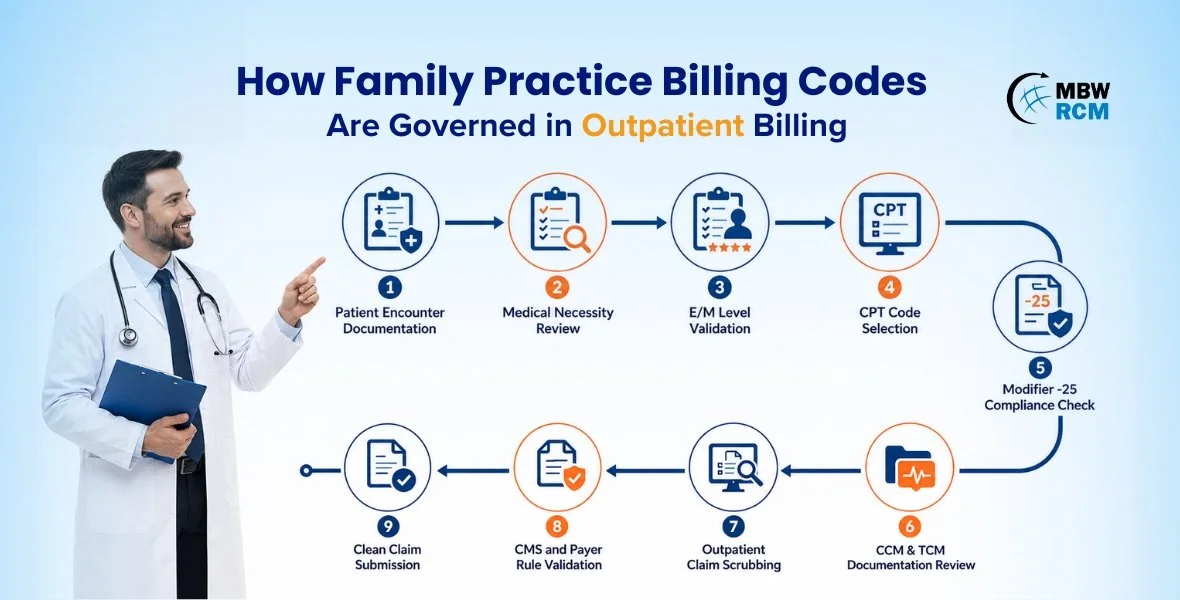
Family medicine outpatient billing involves preventive visits, chronic disease management, same-day E/M reporting, care coordination services, and incident-to supervision workflows that often overlap within a single encounter. Because of this complexity, reporting family practice billing codes requires compliance with CMS outpatient billing regulations and CPT® guidelines.
Many outpatient denials occur due to unsupported E/M levels, incorrect modifier usage, preventive visit overlap, and incomplete CCM documentation.
Below are the five most important outpatient billing rules that govern family practice billing code reporting.
Table of Contents
1. Support 99214 Reporting With Moderate MDM Documentation
CMS outpatient E/M guidelines require family medicine office visit levels to be selected based on:
Medical Decision-Making (MDM),
or total provider time.
Frequently reported family practice billing codes include:
To support 99214 billing, documentation must demonstrate moderate MDM through:
prescription drug management,
multiple chronic condition management,
external lab review,
diagnostic interpretation,
treatment modification,
or elevated patient risk.
Stable chronic condition follow-ups without active physician management typically support only 99213 reporting. Unsupported 99214 utilization remains one of the highest outpatient audit triggers in family medicine reimbursement workflows.
2. Append Modifier -25 Only for Separate E/M Workflows
Modifier -25 allows providers to report:
a preventive service,
minor outpatient procedure,
or diagnostic intervention,
together with a separately identifiable E/M service performed on the same encounter date.
Commonly reported family practice billing codes include:
The additional E/M service must include:
separate physician evaluation,
distinct assessment documentation,
independent medical decision-making,
medically necessary treatment planning.
Payers frequently deny modifier -25 claims when documentation duplicates preventive exam findings or lacks separate problem-oriented physician work.
3. Report Preventive Visits Separately From Chronic Care
Preventive medicine CPT codes include:
annual wellness exams,
preventive screenings,
counseling services,
age-based risk assessments.
These outpatient services do not automatically include:
diabetes management,
hypertension follow-up,
asthma evaluation,
medication adjustments,
chronic condition treatment planning.
Frequently reported preventive family practice billing codes include:
When physicians perform additional chronic disease management during preventive encounters, outpatient E/M services may be separately reported using modifier -25.
Claims involving preventive family practice billing codes are frequently denied when:
chronic conditions are minimally addressed,
treatment changes are absent,
documentation lacks separate medical management workflows.
Clear separation between preventive services and chronic disease evaluation remains essential for outpatient reimbursement compliance.
To understand commonly reported CPT codes in family medicine, check out our blog on “Most Commonly Used Family Practice CPT Codes.”
4. Follow CMS Incident-To Supervision Reporting Standards
CMS incident-to regulations allow outpatient services performed by:
nurse practitioners,
physician assistants,
clinical staff providers
to be billed under the supervising physician’s NPI only when strict supervision requirements are met.
To qualify for incident-to reimbursement:
the physician must establish the original treatment plan,
the patient must remain established,
direct supervision must remain available,
the physician must stay physically present in the office suite.
New patient visits, independently managed complaints, and newly diagnosed conditions do not qualify for incident-to billing. Improper supervision reporting frequently triggers outpatient audit findings and reimbursement recoupments across family medicine billing operations.
5. Maintain CCM and TCM Documentation Compliance Standards
Family medicine providers increasingly report outpatient care coordination services including:
Chronic Care Management (CCM),
Transitional Care Management (TCM).
These services follow strict CMS billing requirements tied to:
patient communication,
time tracking,
care coordination documentation,
post-discharge follow-up timelines.
Frequently reported family practice billing codes include:
CCM reporting requires:
documented patient consent,
minimum monthly time thresholds,
comprehensive care plans,
non-face-to-face coordination documentation.
TCM reporting requires:
patient contact within 2 business days,
medication reconciliation,
follow-up visits within CMS-required timelines.
Missing time logs and incomplete follow-up documentation remain major denial drivers for outpatient care management reimbursement. If you are interested to read more about Family Practice Billing, please have a look at this blog on ‘‘Commonly Used CPT Codes in Family Practice Billing’’.
Solutions for Reducing Outpatient Billing Reporting Errors
Outpatient billing errors in family medicine often result from incorrect E/M reporting, modifier misuse, and documentation gaps. The following are key solutions for reducing outpatient billing reporting errors.
Implement Pre-Bill E/M Scrubbing for 99214 and 99215 Claims
Pre-bill E/M scrubbing tools review:
diagnosis complexity,
prescription management,
risk documentation,
treatment modifications.
Claims lacking moderate or high MDM support are flagged before submission, reducing unsupported:
99214,
99215
reporting errors.
Configure Modifier -25 Edits for Preventive and E/M Encounters
Modifier -25 denials commonly occur when preventive and problem-oriented documentation overlaps within the same outpatient encounter.
Automated billing edits help identify duplicated assessments, missing treatment plans, and incomplete physician work documentation before claim submission. This improves same-day billing accuracy for preventive and E/M reporting.
Use Separate Documentation Templates for Preventive Visits
Separate documentation templates improve reporting accuracy for:
annual wellness visits,
chronic disease management,
medication adjustments,
preventive counseling.
This helps reduce preventive visit overlap errors tied to outpatient family practice billing codes.
Automate CCM and TCM Time Validation Before Claim Submission
CCM and TCM claims frequently fail because monthly time tracking, patient outreach timelines, or medication reconciliation documentation are incomplete.
Automated care management validation workflows help verify required documentation before claim submission, reducing reporting errors involving outpatient care coordination services.
Reducing outpatient billing reporting errors requires stronger coding workflows, compliant documentation, and structured Family Practice Billing for Faster Reimbursements.
Need Help Managing Family Practice Billing Workflows?
E/M reporting errors, modifier -25 issues, and preventive visit overlap can increase outpatient denials. Our family practice billing services help improve billing compliance and reimbursement workflows.
👉 Talk to Our Billing ExpertsConclusion
Understanding outpatient billing rules is essential for accurate reporting of family practice billing codes. Incorrect E/M levels, modifier misuse, preventive visit overlap, and incomplete CCM or TCM documentation continue increasing denials and compliance risk across family medicine billing operations.
Our specialized family practice billing services help healthcare providers strengthen outpatient billing compliance, improve coding accuracy, reduce reporting errors, and optimize reimbursement performance.
Contact MBW RCM today to improve the accuracy and compliance of your family practice billing workflows.
FAQs on Outpatient Billing Rules for Family Practice Billing Codes
Get Expert Help With Outpatient Billing Rules
Incorrect E/M reporting, modifier -25 usage, preventive visit overlap, and incomplete CCM documentation can increase denials and reimbursement delays across family practice billing workflows.
Fill out the form below to improve compliance with outpatient billing rules and reduce reporting errors.